Understand Overpronation Of The Foot
Overview
Over-pronation describes a characteristic gait wherein a lack of sufficient support from the arch of the foot causes it to roll inwards as weight is placed on it. The long arch of the foot is actually a very important structure in terms of our gait and how we walk, it is responsible for ensuring that as our weight rolls from the heel to the balls of our feet it does so in a straight line that doesn?t place undue stress on the ankle or knees. Unfortunately when a person?s arch is not pronounced enough, or even simply not there (a condition called flat footedness), there isn?t enough arch support to maintain a healthy, forward motion of the foot.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
If a young child is diagnosed with overpronation braces and custom orthotics can be, conjunction with strengthening and stretching exercises, to realign the bones of the foot. These treatments may have to continue until the child has stopped growing, and orthotics may need to be worn for life in order to prevent the foot reverting to an overpronated state. Wearing shoes that properly support the foot, particularly the arch, is one of the most effective treatments for overpronation. Custom-made orthotic inserts can also be very beneficial. They too support the arch and distribute body weight correctly throughout the foot. Motion-control shoes that prohibit pronation can be worn, so may be useful for those with severe overpronation. One good treatment is to walk barefoot as often as possible. Not relying on shoes to support the arch will encourage proper muscle use. Practicing yoga can help to correct poor posture and teach you how to stand with your weight balanced evenly across the whole foot.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Over-pronation describes a characteristic gait wherein a lack of sufficient support from the arch of the foot causes it to roll inwards as weight is placed on it. The long arch of the foot is actually a very important structure in terms of our gait and how we walk, it is responsible for ensuring that as our weight rolls from the heel to the balls of our feet it does so in a straight line that doesn?t place undue stress on the ankle or knees. Unfortunately when a person?s arch is not pronounced enough, or even simply not there (a condition called flat footedness), there isn?t enough arch support to maintain a healthy, forward motion of the foot.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
If a young child is diagnosed with overpronation braces and custom orthotics can be, conjunction with strengthening and stretching exercises, to realign the bones of the foot. These treatments may have to continue until the child has stopped growing, and orthotics may need to be worn for life in order to prevent the foot reverting to an overpronated state. Wearing shoes that properly support the foot, particularly the arch, is one of the most effective treatments for overpronation. Custom-made orthotic inserts can also be very beneficial. They too support the arch and distribute body weight correctly throughout the foot. Motion-control shoes that prohibit pronation can be worn, so may be useful for those with severe overpronation. One good treatment is to walk barefoot as often as possible. Not relying on shoes to support the arch will encourage proper muscle use. Practicing yoga can help to correct poor posture and teach you how to stand with your weight balanced evenly across the whole foot.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Calcaneal Apophysitis Physiotherapy
Overview
Foot pain is not only limited to grown-ups. Often, healthy and active children will complain of pain in one or both heels shortly after running, engaging in sports or even walking. The pain is centered at the back of, or under the heel. The cause of heel pain in children is usually a condition called calcaneal apophysitis, normally reported by 8 to 14 year olds.
Causes
Sever condition is caused by sprain injury where the Achilles tendon attaches to the calcaneus bone at the back of the heel. Sever condition occurs in adolescent or older children, particularly active boys. It can be very painful. It is one of those conditions commonly referred to as "growing pains." Patients are evaluated for signs of conditions that can mimic Sever condition, such as ankylosing spondylitis and other forms of arthritis. Usually Sever condition is self-limited; that is, it disappears as the child ages.
Symptoms
This syndrome can occur unilaterally or bilaterally. The incidence of bilaterally is approximately 60%. Common signs and symptoms include posterior inferior heel pain (over the medial and lateral surface of the bone). Pain is usually absent when the child gets up in the morning. Increased pain with weight bearing, running or jumping (= activity-related pain). The area often feels stiff. The child may limp at the end of physical activity. Tenderness at the insertion of the tendons (= an avascular necrosis of the arthropathy). Limited ankle dorsiflexion range secondary to tightness of the Achilles tendon. Hard surfaces and poor-quality or worn-out athletic shoes contribute to increased symptoms. The pain gradually resolves with rest. Reliability or validity of methods used to obtain the ankle joint dorsiflexion or biomechanical malalignment data are not commented upon, thus reducing the quality of the data. Although pain and limping are mentioned as symptomatic traits, there have been no attempts to quantify the pain or its effect on the individual.
Diagnosis
All medical diagnosis should be made by taking a full history, examining the patient then performing investigations. The problem usually occurs in boys who are going through or have just gone through a growth spurt; one or both heels may be affected. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. There may be swelling over the back of the heel and this area is painful if touched or knocked. On examination the patient often has flat feet, very tight legs muscles especially the gastrocnemius.
Non Surgical Treatment
Treatment depends on the severity of the condition, but may include relative rest and modified activity, a physiotherapist can help work out what, and how much, activity to undertake. Cold packs, apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking. Shoe inserts, small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term. Medication, pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor). Anti-inflammatory creams are also an effective management tool. Splinting or casting, in severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare. Time, generally the pain will ease in one to two weeks, although there may be flare-ups from time to time. Correction of any biomechanical issues, a physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition. Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Prevention
The chances of a child developing heel pain can be reduced by avoiding obesity. Choosing well-constructed, supportive shoes that are appropriate for the child?s activity. Avoiding or limiting wearing of cleated athletic shoes. Avoiding activity beyond a child?s ability.
Foot pain is not only limited to grown-ups. Often, healthy and active children will complain of pain in one or both heels shortly after running, engaging in sports or even walking. The pain is centered at the back of, or under the heel. The cause of heel pain in children is usually a condition called calcaneal apophysitis, normally reported by 8 to 14 year olds.
Causes
Sever condition is caused by sprain injury where the Achilles tendon attaches to the calcaneus bone at the back of the heel. Sever condition occurs in adolescent or older children, particularly active boys. It can be very painful. It is one of those conditions commonly referred to as "growing pains." Patients are evaluated for signs of conditions that can mimic Sever condition, such as ankylosing spondylitis and other forms of arthritis. Usually Sever condition is self-limited; that is, it disappears as the child ages.
Symptoms
This syndrome can occur unilaterally or bilaterally. The incidence of bilaterally is approximately 60%. Common signs and symptoms include posterior inferior heel pain (over the medial and lateral surface of the bone). Pain is usually absent when the child gets up in the morning. Increased pain with weight bearing, running or jumping (= activity-related pain). The area often feels stiff. The child may limp at the end of physical activity. Tenderness at the insertion of the tendons (= an avascular necrosis of the arthropathy). Limited ankle dorsiflexion range secondary to tightness of the Achilles tendon. Hard surfaces and poor-quality or worn-out athletic shoes contribute to increased symptoms. The pain gradually resolves with rest. Reliability or validity of methods used to obtain the ankle joint dorsiflexion or biomechanical malalignment data are not commented upon, thus reducing the quality of the data. Although pain and limping are mentioned as symptomatic traits, there have been no attempts to quantify the pain or its effect on the individual.
Diagnosis
All medical diagnosis should be made by taking a full history, examining the patient then performing investigations. The problem usually occurs in boys who are going through or have just gone through a growth spurt; one or both heels may be affected. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. There may be swelling over the back of the heel and this area is painful if touched or knocked. On examination the patient often has flat feet, very tight legs muscles especially the gastrocnemius.
Non Surgical Treatment
Treatment depends on the severity of the condition, but may include relative rest and modified activity, a physiotherapist can help work out what, and how much, activity to undertake. Cold packs, apply ice or cold packs to the back of the heels for around 15 minutes after any physical activity, including walking. Shoe inserts, small heel inserts worn inside the shoes can take some of the traction pressure off the Achilles tendons. This will only be required in the short term. Medication, pain-relieving medication may help in extreme cases, but should always be combined with other treatment and following consultation with your doctor). Anti-inflammatory creams are also an effective management tool. Splinting or casting, in severe cases, it may be necessary to immobilise the lower leg using a splint or cast, but this is rare. Time, generally the pain will ease in one to two weeks, although there may be flare-ups from time to time. Correction of any biomechanical issues, a physiotherapist can identify and discuss any biomechanical issues that may cause or worsen the condition. Education on how to self-manage the symptoms and flare-ups of Sever?s disease is an essential part of the treatment.
Prevention
The chances of a child developing heel pain can be reduced by avoiding obesity. Choosing well-constructed, supportive shoes that are appropriate for the child?s activity. Avoiding or limiting wearing of cleated athletic shoes. Avoiding activity beyond a child?s ability.
Tibial Posterior Tendon Dysfunction Stages
Overview
Adult-acquired flatfoot is a challenging condition to treat. It is defined as a symptomatic, progressive deformity of the foot caused by loss of supportive structures of the medial arch. It is becoming increasingly frequent with the aging population and the obesity epidemic. Patients commonly try to lose weight by exercising to improve the condition. This often leads to worsening of symptoms and progression of the disorder. Early recognition of this complex disorder is essential, if chronic pain and surgery are to be avoided. 
Causes
Several risk factors are associated with PTT dysfunction, including high blood pressure, obesity, diabetes, previous ankle surgery or trauma and exposure to steroids. A person who suspects that they are suffering from PTT dysfunction should seek medical attention earlier rather than later. It is much easier to treat early and avoid a collapsed arch than it is to repair one. When the pain first happens and there is no significant flatfoot deformity, initial treatments include rest, oral anti-inflammatory medications and, depending on the severity, a special boot or brace.
Symptoms
Pain and swelling around the inside aspect of the ankle initially. Later, the arch of the foot may fall (foot becomes flat), this change leads to walking to become difficult and painful, as well as standing for long periods. As the flat foot becomes established, pain may progress to the outer part of the ankle. Eventually, arthritis may develop.
Diagnosis
Observation by a skilled foot clinician and a hands-on evaluation of the foot and ankle is the most accurate diagnostic technique. Your Dallas foot doctor may have you do a walking examination (the most reliable way to check for the deformity). During walking, the affected foot appears more pronated and deformed. Your podiatrist may do muscle testing to look for strength deficiencies. During a single foot raise test, the foot doctor will ask you to rise up on the tip of your toes while keeping your unaffected foot off the ground. If your posterior tendon has been attenuated or ruptured, you will be unable to lift your heel off the floor. In less severe cases, it is possible to rise onto your toes, but your heel will not invert normally. X-rays are not always helpful as a diagnostic tool for Adult Flatfoot because both feet will generally demonstrate a deformity. MRI (magnetic resonance imaging) may show tendon injury and inflammation, but can?t always be relied on for a complete diagnosis. In most cases, a MRI is not necessary to diagnose a posterior tibial tendon injury. An ultrasound may also be used to confirm the deformity, but is usually not required for an initial diagnosis.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. 
Surgical Treatment
For those patients with PTTD that have severe deformity or have not improved with conservative treatments, surgery may be necessary to return them to daily activity. Surgery for PTTD may include repair of the diseased tendon and possible tendon transfer to a nearby healthy tendon, surgery on the surrounding bones or joints to prevent biomechanical abnormalities that may be a contributing factor or both.
All The Things You Will Need To Understand About Heel Pain
Overview

Plantar fasciitis is a painful condition affecting the bottom of the foot. It is a common cause of Heel Pain and is sometimes called a heel spur. Plantar fasciitis is the correct term to use when there is active inflammation. Plantar fasciosis is more accurate when there is no inflammation but chronic degeneration instead. Acute plantar fasciitis is defined as inflammation of the origin of the plantar fascia and fascial structures around the area. Plantar fasciitis or fasciosis is usually just on one side. In about 30 per cent of all cases, both feet are affected. This guide will help you understand how plantar fasciitis develops, how the condition causes problems, what can be done for your pain.
Causes
Heel pain can have many causes. If your heel hurts, see your primary care doctor or orthopaedic foot and ankle specialist right away to determine why and get treatment. Tell him or her exactly where you have pain and how long you've had it. Your doctor will examine your heel, looking and feeling for signs of tenderness and swelling. You may be asked to walk, stand on one foot or do other physical tests that help your doctor pinpoint the cause of your sore heel. Conditions that cause heel pain generally fall into two main categories: pain beneath the heel and pain behind the heel.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
The following steps may help relieve your heel pain. Use crutches to take weight off your feet. Rest as much as possible for at least a week. Apply ice to the painful area. Do this at least twice a day for 10 to 15 minutes, more often in the first couple of days. Take acetaminophen or ibuprofen for pain. Wear proper-fitting shoes. Use a heel cup, felt pads in the heel area, or shoe insert. Wear night splints. Your doctor may recommend other treatments, depending on the cause of your heel pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention

Wear properly fitting shoes. Place insoles or inserts in your shoes to help control abnormal foot motion. Maintain a healthy weight. Exercise and do foot stretches as they have been shown to decrease the incidence of heel pain.
Plantar fasciitis is a painful condition affecting the bottom of the foot. It is a common cause of Heel Pain and is sometimes called a heel spur. Plantar fasciitis is the correct term to use when there is active inflammation. Plantar fasciosis is more accurate when there is no inflammation but chronic degeneration instead. Acute plantar fasciitis is defined as inflammation of the origin of the plantar fascia and fascial structures around the area. Plantar fasciitis or fasciosis is usually just on one side. In about 30 per cent of all cases, both feet are affected. This guide will help you understand how plantar fasciitis develops, how the condition causes problems, what can be done for your pain.
Causes
Heel pain can have many causes. If your heel hurts, see your primary care doctor or orthopaedic foot and ankle specialist right away to determine why and get treatment. Tell him or her exactly where you have pain and how long you've had it. Your doctor will examine your heel, looking and feeling for signs of tenderness and swelling. You may be asked to walk, stand on one foot or do other physical tests that help your doctor pinpoint the cause of your sore heel. Conditions that cause heel pain generally fall into two main categories: pain beneath the heel and pain behind the heel.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
The following steps may help relieve your heel pain. Use crutches to take weight off your feet. Rest as much as possible for at least a week. Apply ice to the painful area. Do this at least twice a day for 10 to 15 minutes, more often in the first couple of days. Take acetaminophen or ibuprofen for pain. Wear proper-fitting shoes. Use a heel cup, felt pads in the heel area, or shoe insert. Wear night splints. Your doctor may recommend other treatments, depending on the cause of your heel pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention
Wear properly fitting shoes. Place insoles or inserts in your shoes to help control abnormal foot motion. Maintain a healthy weight. Exercise and do foot stretches as they have been shown to decrease the incidence of heel pain.
The Main Causes And Treatment Plans For Achilles Tendonitis Suffering
Overview
 The Achilles is a large tendon that connects two major calf muscles to the back of the heel bone. If this tendon is overworked and tightens, the collagen fibres of the tendon may break, causing inflammation and pain. This can result in scar tissue formation, a type of tissue that does not have the flexibility of tendon tissue. Four types of Achilles injuries exist, 1) Paratendonitis - involves a crackly or crepitus feeling in the tissues surrounding the Achilles tendon. 2) Proliferative Tendinitis - the Achilles tendon thickens as a result of high tension placed on it. 3) Degenerative Tendinitis - a chronic condition where the Achilles tendon is permanently damaged and does not regain its structure. 4) Enthesis - an inflammation at the point where the Achilles tendon inserts into the heel bone.
The Achilles is a large tendon that connects two major calf muscles to the back of the heel bone. If this tendon is overworked and tightens, the collagen fibres of the tendon may break, causing inflammation and pain. This can result in scar tissue formation, a type of tissue that does not have the flexibility of tendon tissue. Four types of Achilles injuries exist, 1) Paratendonitis - involves a crackly or crepitus feeling in the tissues surrounding the Achilles tendon. 2) Proliferative Tendinitis - the Achilles tendon thickens as a result of high tension placed on it. 3) Degenerative Tendinitis - a chronic condition where the Achilles tendon is permanently damaged and does not regain its structure. 4) Enthesis - an inflammation at the point where the Achilles tendon inserts into the heel bone.
Causes
Achilles tendinitis can be caused by any activity that puts stress on your Achilles tendon. Tendinitis can develop if you run or jump more than usual or exercise on a hard surface. Tendinitis can be caused by shoes that do not fit or support your foot and ankle. Tight tendons and muscles, You may have tight hamstring and calf muscles in your upper and lower leg. Your tendons also become stiffer and easier to injure as you get older. Arthritis, Bony growths caused by arthritis can irritate the Achilles tendon, especially around your heel.
Symptoms
If you have Achilles tendinitis or Achilles enthesopathy, you are likely to experience the following symptoms. Pain. You may notice aching, burning, or tearing pains at the back of your heel or above the ankle. The pain can range from mild to very severe and disabling. It is most noticeable in the following circumstances. After resting. Many people report that pain increases when they first get out of bed in the morning or after sitting for a period of time. After exercise. Pain may increase if you exercise or stand for a period of time. A lump. In some cases, a tender lump can develop at the site of the injured tendon (tendinosis). Bone spurs. When the injury occurs at the point where the tendon attaches to the foot, a bone spur may develop on the heel.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
The recommended treatment for Achilles tendinitis consists of icing, gentle stretching, and modifying or limiting activity. Nonsteroidal anti-inflammatory medications (NSAIDs), such as ibuprofen or aspirin, can reduce pain and swelling. Physical therapy and the use of an orthotic (heel lift) can also be helpful. For chronic cases where tendinosis is evident and other methods of treatment have failed, surgery may be recommended to remove and repair the damaged tissue.

Surgical Treatment
Surgery is considered the last resort and is often performed by an orthopedic surgeon. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
The Achilles is a large tendon that connects two major calf muscles to the back of the heel bone. If this tendon is overworked and tightens, the collagen fibres of the tendon may break, causing inflammation and pain. This can result in scar tissue formation, a type of tissue that does not have the flexibility of tendon tissue. Four types of Achilles injuries exist, 1) Paratendonitis - involves a crackly or crepitus feeling in the tissues surrounding the Achilles tendon. 2) Proliferative Tendinitis - the Achilles tendon thickens as a result of high tension placed on it. 3) Degenerative Tendinitis - a chronic condition where the Achilles tendon is permanently damaged and does not regain its structure. 4) Enthesis - an inflammation at the point where the Achilles tendon inserts into the heel bone.
Causes
Achilles tendinitis can be caused by any activity that puts stress on your Achilles tendon. Tendinitis can develop if you run or jump more than usual or exercise on a hard surface. Tendinitis can be caused by shoes that do not fit or support your foot and ankle. Tight tendons and muscles, You may have tight hamstring and calf muscles in your upper and lower leg. Your tendons also become stiffer and easier to injure as you get older. Arthritis, Bony growths caused by arthritis can irritate the Achilles tendon, especially around your heel.
Symptoms
If you have Achilles tendinitis or Achilles enthesopathy, you are likely to experience the following symptoms. Pain. You may notice aching, burning, or tearing pains at the back of your heel or above the ankle. The pain can range from mild to very severe and disabling. It is most noticeable in the following circumstances. After resting. Many people report that pain increases when they first get out of bed in the morning or after sitting for a period of time. After exercise. Pain may increase if you exercise or stand for a period of time. A lump. In some cases, a tender lump can develop at the site of the injured tendon (tendinosis). Bone spurs. When the injury occurs at the point where the tendon attaches to the foot, a bone spur may develop on the heel.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
The recommended treatment for Achilles tendinitis consists of icing, gentle stretching, and modifying or limiting activity. Nonsteroidal anti-inflammatory medications (NSAIDs), such as ibuprofen or aspirin, can reduce pain and swelling. Physical therapy and the use of an orthotic (heel lift) can also be helpful. For chronic cases where tendinosis is evident and other methods of treatment have failed, surgery may be recommended to remove and repair the damaged tissue.
Surgical Treatment
Surgery is considered the last resort and is often performed by an orthopedic surgeon. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
What Is Pain In The Heel And Tips To Remedy It

Overview
Plantar Fasciitis is a painful foot condition that affects the Plantar Fascia tendon that runs along the bottom of the foot (as seen in the picture). This tendon runs along the arches of the foot. Sometimes this tendon can become sore from normal use or strenuous activity, but this is not to be confused with the pain associated with Plantar Fasciitis. Small tears in the plantar fascia tendon can cause foot discomfort and pain, if left untreated, can become unbearable (seen in picture below). These tears are made worse by over-use, strenuous activity, weight gain, improper foot wear and a variety of other factors. Although there is no one absolute cause for the condition, it remains clear that this condition, while painful, can be corrected with products such as footwear, night splints, insoles and a variety of other plantar fasaciitis products.
Causes
As a person gets older, the plantar fascia becomes less like a rubber band and more like a rope that doesn't stretch very well. The fat pad on the heel becomes thinner and can't absorb as much of the shock caused by walking. The extra shock damages the plantar fascia and may cause it to swell, tear or bruise. You may notice a bruise or swelling on your heel. Other risk factors for plantar fasciitis include being overweight and obesity. Diabetes. Spending most of the day on your feet. Becoming very active in a short period of time. Being flat-footed or having a high arch.
Symptoms
The condition typically starts gradually with mild pain at the heel bone often referred to as a stone bruise. You're more likely to feel it after (not during) exercise. The pain classically occurs right after getting up in the morning and after a period of sitting. If you don't treat plantar fasciitis, it may become a chronic condition. You may not be able to keep up your level of activity, and you may develop symptoms of foot, knee, hip and back problems because plantar fasciitis can change the way you walk.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
At the first sign of soreness, massage (roll a golf ball under your foot) and apply ice (roll a frozen bottle of water under your foot). What you wear on your feet when you're not running makes a difference. Arch support is key, and walking around barefoot or in flimsy shoes can delay recovery. If pain is present for more than three weeks, see a sports podiatrist. Treatments such as orthotics, foot taping, cortisone injections, night splints, and anti-inflammatories decrease symptoms significantly in about 95 percent of sufferers within six weeks. For more stubborn cases, physical therapy may be prescribed; six months of chronic pain may benefit from shock-wave therapy, an FDA-approved plantar-fasciitis treatment.

Surgical Treatment
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.
What Causes Heel Discomfort To Flare Up
Overview
Plantar Fasciitis is a painful foot condition that affects the Plantar Fascia tendon that runs along the bottom of the foot (as seen in the picture). This tendon runs along the arches of the foot. Sometimes this tendon can become sore from normal use or strenuous activity, but this is not to be confused with the pain associated with Plantar Fasciitis. Small tears in the plantar fascia tendon can cause foot discomfort and pain, if left untreated, can become unbearable (seen in picture below). These tears are made worse by over-use, strenuous activity, weight gain, improper foot wear and a variety of other factors. Although there is no one absolute cause for the condition, it remains clear that this condition, while painful, can be corrected with products such as footwear, night splints, insoles and a variety of other plantar fasaciitis products.
Causes
Plantar fasciitis is one of those injuries that magically seems to appear for no apparent reason. However, plantar fasciitis is caused by one of two methods. They are either traction or compression injuries. Plantar fasciitis is most often associated with impact and running sports, especially those that involve toe running rather than heel running styles. It is also commonly diagnosed in individuals with poor foot biomechanics that stress the plantar fascia. Flat feet or weak foot arch control muscles are two common causes of plantar fasciitis.
Symptoms
People with this condition sometimes describe the feeling as a hot, sharp sensation in the heel. You usually notice the pain first thing in the morning when you stand. After walking for a period of time, the pain usually lessens or even disappears. However, sharp pain in the center of the heel may return after resting for a period of time and then resuming activity.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
Treatments you can do at home include rest. Try to avoid activities that put stress on your feet. This can be hard, especially if your job involves being on your feet for hours at a time, but giving your feet as much rest as possible is the first step in reducing the pain of plantar fasciitis. Use ice or a cold compress to reduce pain and inflammation. Do this three or four times a day for about 20 minutes at a time until the pain goes away. Take anti-inflammatory medications. Painkillers such as ibuprofen or acetaminophen can help relieve pain and reduce inflammation in the affected area. Your doctor may also prescribe a medication called a corticosteroid to help treat severe pain. Exercise your feet and calves. When the pain is gone, do calf and foot stretches and leg exercises to make your legs as strong and flexible as possible. This can help you avoid getting plantar fasciitis again. Ask your coach, athletic trainer, or a physical therapist to show you some leg exercises. Rolling a tennis ball under your foot can massage the area and help the injury heal. Talk to your doctor about shoe inserts or night splints. Shoe inserts can give your feet added support to aid in the healing process. Night splints keep your calf muscles gently flexed, helping to keep your plantar fascia from tightening up overnight. Have a trainer or sports injury professional show you how to tape your foot. A proper taping job allows your plantar fascia to get more rest. You should tape your foot each time you exercise until the pain is completely gone. For people who get repeated sports injuries, it can help to see a sports medicine specialist. These experts are trained in evaluating things like an athlete's running style, jumping stance, or other key moves. They can teach you how to make the most of your body's strengths and compensate for any weaknesses. Once you're healed, look for the silver lining in your bench time. You may find that what you learn from having an injury leads you to play a better game than ever before.

Surgical Treatment
Plantar fasciotomy is often considered after conservative treatment has failed to resolve the issue after six months and is viewed as a last resort. Minimally invasive and endoscopic approaches to plantar fasciotomy exist but require a specialist who is familiar with certain equipment. Heel spur removal during plantar fasciotomy has not been found to improve the surgical outcome. Plantar heel pain may occur for multiple reasons and release of the lateral plantar nerve branch may be performed alongside the plantar fasciotomy in select cases. Possible complications of plantar fasciotomy include nerve injury, instability of the medial longitudinal arch of the foot, fracture of the calcaneus, prolonged recovery time, infection, rupture of the plantar fascia, and failure to improve the pain. Coblation (TOPAZ) surgery has recently been proposed as alternative surgical approaches for the treatment of recalcitrant plantar fasciitis.
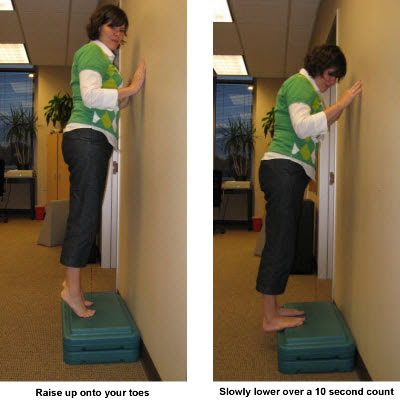
Stretching Exercises
Stretching exercises for your foot are important. Do the stretches shown here at least twice a day. Don't bounce when you stretch. Plantar fascia stretch. To do the plantar fascia stretch, stand straight with your hands against a wall and your injured leg slightly behind your other leg. Keeping your heels flat on the floor, slowly bend both knees. You should feel the stretch in the lower part of your leg. Hold the stretch for 10 to 15 seconds. Repeat the stretch 6 to 8 times. Calf stretch. Stand with your hands against a wall and your injured leg behind your other leg. With your injured leg straight, your heel flat on the floor and your foot pointed straight ahead, lean slowly forward, bending the other leg. You should feel the stretch in the middle of your calf. Hold the stretch for 10 to 15 seconds. Repeat the stretch 6 to 8 times. Other exercises. You can also strengthen your leg muscles by standing on the ball of your foot at the edge of a step and raising up as high as possible on your toes. Relax between toe raises and let your heel fall a little lower than the edge of the step. It's also helpful to strengthen the foot by grabbing a towel with your toes as if you are going to pick up the towel with your foot. Repeat this exercise several times a day.