Techniques To Manage Fallen Arches
Overview

Fallen arches, also called flat feet or pes planus, is a condition in which the entire bottom of the foot touches the ground when a person is standing. A normal foot has an arch between the heel and the ball of the foot. Fallen arches are typically an acquired condition, though flat feet may be present from childhood if the arch never developed in the first place. In some cases, usually those in which the arch never developed, flat feet are not a cause for concern. If they develop in adulthood, however, causing a rigid flat foot, the condition is usually accompanied by pain and can cause serious health issues.
Causes
You can have a tendency towards fallen arches from birth. Up through the toddler stage, it is common to have flat feet. Throughout childhood, arches tend to normally develop. For reasons not well understood, however, in some cases the feet stay flat and the arch never forms. In many cases this abnormality does not cause symptoms or require any treatment. In other cases, it is due to a condition called tarsal coalition. This occurs when some of the foot bones fuse.
Symptoms
Having flat feet can be painless and is actually normal in some people. But others with flat feet experience pain in the heel or arch area, difficulty standing on tiptoe, or have swelling along the inside of the ankle. They may also experience pain after standing for long periods of time or playing sports. Some back problems can also be attributed to flat feet.
Diagnosis
Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis.
arch support inserts reviews
Non Surgical Treatment
If you have flat feet (pes planus) it does not mean you will have problems or pain. Flat feet are a common condition. Flat feet are defined as an abnormal lowering of the medial longitudinal arch. There is often a hereditary component to the development of flat feet. Flat feet are more common in certain ethnic groups. Flat feet usually occurs equally in both feet and become apparent at an early age. Flat feet can initially be asymptomatic, but can become progressively symptomatic with age. Some flat feet never become bothersome. The medial arch is unstable in flexible flatfoot. The foot can bend as the heel lifts of the ground. This creates stress on the surrounding soft-tissues and joints creating tired, sore arches. The instability of the foot can create abnormal stress that flows up the leg which results in pain in the legs, knees, hips and lower back. Patients with flat feet often present to the chiropodist/podiatrist with problems that are indirectly caused by their foot structure.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Fallen arches, also called flat feet or pes planus, is a condition in which the entire bottom of the foot touches the ground when a person is standing. A normal foot has an arch between the heel and the ball of the foot. Fallen arches are typically an acquired condition, though flat feet may be present from childhood if the arch never developed in the first place. In some cases, usually those in which the arch never developed, flat feet are not a cause for concern. If they develop in adulthood, however, causing a rigid flat foot, the condition is usually accompanied by pain and can cause serious health issues.
Causes
You can have a tendency towards fallen arches from birth. Up through the toddler stage, it is common to have flat feet. Throughout childhood, arches tend to normally develop. For reasons not well understood, however, in some cases the feet stay flat and the arch never forms. In many cases this abnormality does not cause symptoms or require any treatment. In other cases, it is due to a condition called tarsal coalition. This occurs when some of the foot bones fuse.
Symptoms
Having flat feet can be painless and is actually normal in some people. But others with flat feet experience pain in the heel or arch area, difficulty standing on tiptoe, or have swelling along the inside of the ankle. They may also experience pain after standing for long periods of time or playing sports. Some back problems can also be attributed to flat feet.
Diagnosis
Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis.
arch support inserts reviews
Non Surgical Treatment
If you have flat feet (pes planus) it does not mean you will have problems or pain. Flat feet are a common condition. Flat feet are defined as an abnormal lowering of the medial longitudinal arch. There is often a hereditary component to the development of flat feet. Flat feet are more common in certain ethnic groups. Flat feet usually occurs equally in both feet and become apparent at an early age. Flat feet can initially be asymptomatic, but can become progressively symptomatic with age. Some flat feet never become bothersome. The medial arch is unstable in flexible flatfoot. The foot can bend as the heel lifts of the ground. This creates stress on the surrounding soft-tissues and joints creating tired, sore arches. The instability of the foot can create abnormal stress that flows up the leg which results in pain in the legs, knees, hips and lower back. Patients with flat feet often present to the chiropodist/podiatrist with problems that are indirectly caused by their foot structure.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Do You Understand Heel Pain?
Overview
One of the most common foot problems seen by physicians is heel pain. Heel pain that occurs in adult patients is most commonly caused by a condition known as plantar fasciitis. This condition is sometimes also known as a heel spur. Heel pain can also be caused by other factors, such as stress fracture, tendinitis, arthritis, nerve entrapment, cyst in the heel bone.
Causes
Age plays a large role in the development of heel pain, particularly among those over 40. Being active is also a common factor of heel pain. Over time, the elasticity of the tissue in our feet decreases with age, causing us to become prone to damage and also slowing the body's ability to heal damage. Adolescents are also not immune to heel pain. Those who are active in sports are particularly prone to excessively stretching or straining the plantar fascia or Achilles tendon, causing severe heel pain. In most cases, heel pain develops in only one heel. There are many risk factors that lead to heel pain. Abnormal gait and excessive, repetitive stress are common factors in the development of pain and damage. Among the other risk factors involved with the development of heel pain are repetitive exercise or activities, such as long distance running or jumping from activities such as basketball. Obesity. Walking barefoot on hard surfaces. Prolonged standing. Wearing poor fitting shoes, or shoes that do not provide enough support or cushioning. Not stretching properly or at all before and after exercise. Those who are on their feet for long periods of time.
Symptoms
The heel can be painful in many different ways, depending on the cause. Plantar fasciitis commonly causes intense heel pain along the bottom of the foot during the first few steps after getting out of bed in the morning. This heel pain often goes away once you start to walk around, but it may return in the late afternoon or evening. Although X-ray evidence suggests that about 10% of the general population has heels spurs, many of these people do not have any symptoms. In others, heel spurs cause pain and tenderness on the undersurface of the heel that worsen over several months. In a child, this condition causes pain and tenderness at the lower back portion of the heel. The affected heel is often sore to the touch but not obviously swollen. Bursitis involving the heel causes pain in the middle of the undersurface of the heel that worsens with prolonged standing and pain at the back of the heel that worsens if you bend your foot up or down. Pump bump, this condition causes a painful enlargement at the back of the heel, especially when wearing shoes that press against the back of the heel. Heel bruises, like bruises elsewhere in the body, may cause pain, mild swelling, soreness and a black-and-blue discoloration of the skin. Achilles tendonitis, this condition causes pain at the back of the heel where the Achilles tendon attaches to the heel. The pain typically becomes worse if you exercise or play sports, and it often is followed by soreness, stiffness and mild swelling. A trapped nerve can cause pain, numbness or tingling almost anywhere at the back, inside or undersurface of the heel. In addition, there are often other symptoms, such as swelling or discoloration - if the trapped nerve was caused by a sprain, fracture or other injury.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
If the plantar fasciitis is acute, that is, a sprain of the plantar fascia then it is basically treated as a sprain, with anti-inflammatory drugs, ice, rest, possibly physical therapy. If chronic, the poor foot mechanics need be addressed. Foot mechanics are changed by use of specially moulded shoe inserts known as orthotics. Someone with plantar fasciitis needs an orthotic designed to relieve strain on the plantar fascia. Orthotics are often confused with arch supports. Arch supports, by holding up the arch can remove some of the tension from the plantar fascia. Orthotics, on the other hand, do most of their work on the heel and ball of the foot repositioning the foot for maximized function. What can you do before you see the foot doctor? First, try doing your own version of deep tissue massage by rolling a frozen cola bottle or can from the heel forward into the arch. Do it gently. Do stretching but the key to good stretching is not to stretch too hard so generally avoid weight bearing (standing) stretches but sit on a soft surface like your bed and pull the foot backward on the leg as far as it will go, holding for 20 seconds and relaxing for 5 seconds. Each 25 second ?set? can be repeated 5 times and you have invested about 2 minutes in giving yourself a lot of help. Watch out for the shoes you wear. It is tempting to obtain shoes that are colorful and soft. Here is the proof that soft shoes are bad. Wrap a pillow around your foot with duct tape and walk for a block or two. You will come back with your foot hurting more because your foot sank down deeper into the soft surface, allowing the ligament to stretch more. The shoes should be stiff in the shank and flexible at the ball. Such shoes, to running buffs, are known as motion control shoes or stability shoes so going to one of the small specialty running shoes stores is a good place to start. If you don?t have a desk job, or have an industrial job see if light duty is available. A note from your doc may be all that is required in most cases and most doctors are happy to oblige.
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
heel cups for achilles tendonitis
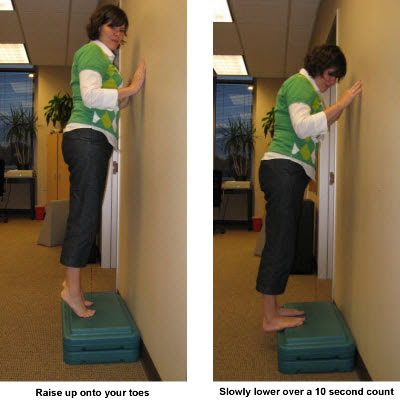
Prevention

The following steps will help prevent plantar fasciitis or help keep the condition from getting worse if you already have it. The primary treatment is rest. Cold packs application to the area for 20 minutes several times a day or after activities give some relief. Over-the-counter pain medications can help manage the pain, consult your healthcare professional. Shoes should be well cushioned, especially in the midsole area, and should have the appropriate arch support. Some will benefit from an orthotic shoe insert, such as a rubber heel pad for cushioning. Orthotics should be used in both shoes, even if only one foot hurts. Going barefoot or wearing slipper puts stress on your feet. Put on supportive shoes as soon as you get out of bed. Calf stretches and stretches using a towel (place the towel under the ball of your feet and pull gently the towel toward you and hold a few seconds) several times a day, especially when first getting up in the morning. Stretching the Achilles tendon at the back of the heel is especially important before sports, but it is helpful for nonathletes as well. Increasing your exercise levels gradually. Staying at a healthy weight. Surgery is very rarely required.
One of the most common foot problems seen by physicians is heel pain. Heel pain that occurs in adult patients is most commonly caused by a condition known as plantar fasciitis. This condition is sometimes also known as a heel spur. Heel pain can also be caused by other factors, such as stress fracture, tendinitis, arthritis, nerve entrapment, cyst in the heel bone.
Causes
Age plays a large role in the development of heel pain, particularly among those over 40. Being active is also a common factor of heel pain. Over time, the elasticity of the tissue in our feet decreases with age, causing us to become prone to damage and also slowing the body's ability to heal damage. Adolescents are also not immune to heel pain. Those who are active in sports are particularly prone to excessively stretching or straining the plantar fascia or Achilles tendon, causing severe heel pain. In most cases, heel pain develops in only one heel. There are many risk factors that lead to heel pain. Abnormal gait and excessive, repetitive stress are common factors in the development of pain and damage. Among the other risk factors involved with the development of heel pain are repetitive exercise or activities, such as long distance running or jumping from activities such as basketball. Obesity. Walking barefoot on hard surfaces. Prolonged standing. Wearing poor fitting shoes, or shoes that do not provide enough support or cushioning. Not stretching properly or at all before and after exercise. Those who are on their feet for long periods of time.
Symptoms
The heel can be painful in many different ways, depending on the cause. Plantar fasciitis commonly causes intense heel pain along the bottom of the foot during the first few steps after getting out of bed in the morning. This heel pain often goes away once you start to walk around, but it may return in the late afternoon or evening. Although X-ray evidence suggests that about 10% of the general population has heels spurs, many of these people do not have any symptoms. In others, heel spurs cause pain and tenderness on the undersurface of the heel that worsen over several months. In a child, this condition causes pain and tenderness at the lower back portion of the heel. The affected heel is often sore to the touch but not obviously swollen. Bursitis involving the heel causes pain in the middle of the undersurface of the heel that worsens with prolonged standing and pain at the back of the heel that worsens if you bend your foot up or down. Pump bump, this condition causes a painful enlargement at the back of the heel, especially when wearing shoes that press against the back of the heel. Heel bruises, like bruises elsewhere in the body, may cause pain, mild swelling, soreness and a black-and-blue discoloration of the skin. Achilles tendonitis, this condition causes pain at the back of the heel where the Achilles tendon attaches to the heel. The pain typically becomes worse if you exercise or play sports, and it often is followed by soreness, stiffness and mild swelling. A trapped nerve can cause pain, numbness or tingling almost anywhere at the back, inside or undersurface of the heel. In addition, there are often other symptoms, such as swelling or discoloration - if the trapped nerve was caused by a sprain, fracture or other injury.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
If the plantar fasciitis is acute, that is, a sprain of the plantar fascia then it is basically treated as a sprain, with anti-inflammatory drugs, ice, rest, possibly physical therapy. If chronic, the poor foot mechanics need be addressed. Foot mechanics are changed by use of specially moulded shoe inserts known as orthotics. Someone with plantar fasciitis needs an orthotic designed to relieve strain on the plantar fascia. Orthotics are often confused with arch supports. Arch supports, by holding up the arch can remove some of the tension from the plantar fascia. Orthotics, on the other hand, do most of their work on the heel and ball of the foot repositioning the foot for maximized function. What can you do before you see the foot doctor? First, try doing your own version of deep tissue massage by rolling a frozen cola bottle or can from the heel forward into the arch. Do it gently. Do stretching but the key to good stretching is not to stretch too hard so generally avoid weight bearing (standing) stretches but sit on a soft surface like your bed and pull the foot backward on the leg as far as it will go, holding for 20 seconds and relaxing for 5 seconds. Each 25 second ?set? can be repeated 5 times and you have invested about 2 minutes in giving yourself a lot of help. Watch out for the shoes you wear. It is tempting to obtain shoes that are colorful and soft. Here is the proof that soft shoes are bad. Wrap a pillow around your foot with duct tape and walk for a block or two. You will come back with your foot hurting more because your foot sank down deeper into the soft surface, allowing the ligament to stretch more. The shoes should be stiff in the shank and flexible at the ball. Such shoes, to running buffs, are known as motion control shoes or stability shoes so going to one of the small specialty running shoes stores is a good place to start. If you don?t have a desk job, or have an industrial job see if light duty is available. A note from your doc may be all that is required in most cases and most doctors are happy to oblige.
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
heel cups for achilles tendonitis
Prevention
The following steps will help prevent plantar fasciitis or help keep the condition from getting worse if you already have it. The primary treatment is rest. Cold packs application to the area for 20 minutes several times a day or after activities give some relief. Over-the-counter pain medications can help manage the pain, consult your healthcare professional. Shoes should be well cushioned, especially in the midsole area, and should have the appropriate arch support. Some will benefit from an orthotic shoe insert, such as a rubber heel pad for cushioning. Orthotics should be used in both shoes, even if only one foot hurts. Going barefoot or wearing slipper puts stress on your feet. Put on supportive shoes as soon as you get out of bed. Calf stretches and stretches using a towel (place the towel under the ball of your feet and pull gently the towel toward you and hold a few seconds) several times a day, especially when first getting up in the morning. Stretching the Achilles tendon at the back of the heel is especially important before sports, but it is helpful for nonathletes as well. Increasing your exercise levels gradually. Staying at a healthy weight. Surgery is very rarely required.
Functional Leg Length Discrepancy Causes
Overview
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment depends on the amount and cause of the leg length discrepancy as well as the age of your child. Typically, if the difference is less than 2 cm we don?t recommend immediate treatment. We may recommend that your child wear a heel lift in one shoe to make walking and running more comfortable. If the leg length discrepancy is more significant, your doctor may recommend surgery to shorten or lengthen a leg. The procedure used most often to shorten a leg is called epiphysiodesis.

leg length discrepancy symptoms
Surgical Treatment
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment depends on the amount and cause of the leg length discrepancy as well as the age of your child. Typically, if the difference is less than 2 cm we don?t recommend immediate treatment. We may recommend that your child wear a heel lift in one shoe to make walking and running more comfortable. If the leg length discrepancy is more significant, your doctor may recommend surgery to shorten or lengthen a leg. The procedure used most often to shorten a leg is called epiphysiodesis.
leg length discrepancy symptoms
Surgical Treatment
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Leg Length Discrepancy Heel Lifts
Overview
Leg length discrepancies are differences between the lengths of your legs. Not only can the actual difference vary from person to person but also how much it affects daily life. Small discrepancies often go unnoticed and do not need to be treated. Larger differences may affect posture or cause a limp during walking. The discrepancy may be from the upper leg bone (femur) or the lower leg bone (tibia).
Causes
Sometimes the cause of LLD is unknown, yet the pattern or combination of conditions is consistent with a certain abnormality. Examples include underdevelopment of the inner or outer side of the leg (hemimelias) or (partial) inhibition of growth of one side of the body of unknown cause (hemihypertrophy). These conditions are present at birth, but the limb length difference may be too small to be detected. As the child grows, the LLD increases and becomes more noticeable. In hemimelia, one of the two bones between the knee and the ankle (tibia or fibula) is abnormally short. There also may be associated foot or knee abnormalities. Hemihypertrophy or hemiatrophy are rare conditions in which there is a difference in length of both the arm and leg on only one side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This type of limb length is called idiopathic. While there is a cause, it cannot be determined using currect diagnostic methods.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.

what happens if one leg is shorter than the other?
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Leg length discrepancies are differences between the lengths of your legs. Not only can the actual difference vary from person to person but also how much it affects daily life. Small discrepancies often go unnoticed and do not need to be treated. Larger differences may affect posture or cause a limp during walking. The discrepancy may be from the upper leg bone (femur) or the lower leg bone (tibia).
Causes
Sometimes the cause of LLD is unknown, yet the pattern or combination of conditions is consistent with a certain abnormality. Examples include underdevelopment of the inner or outer side of the leg (hemimelias) or (partial) inhibition of growth of one side of the body of unknown cause (hemihypertrophy). These conditions are present at birth, but the limb length difference may be too small to be detected. As the child grows, the LLD increases and becomes more noticeable. In hemimelia, one of the two bones between the knee and the ankle (tibia or fibula) is abnormally short. There also may be associated foot or knee abnormalities. Hemihypertrophy or hemiatrophy are rare conditions in which there is a difference in length of both the arm and leg on only one side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This type of limb length is called idiopathic. While there is a cause, it cannot be determined using currect diagnostic methods.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.
what happens if one leg is shorter than the other?
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
What Causes Mortons Neuroma
Overview
 The nerves located on the bottom of the foot between the metatarsal heads (the bone of the toe closest to the foot) supply feeling, or sensation, to the toes. One of these nerves may become irritated by the ligament located above it, causing it to become thickened and painful. Generally this problem occurs most often between the third and fourth toes, but it can occur between the second and third toes as well. It is uncommon for a neuroma to be located between the first and second or fourth and fifth metatarsals. Rarely is there more than one neuroma in a foot.
The nerves located on the bottom of the foot between the metatarsal heads (the bone of the toe closest to the foot) supply feeling, or sensation, to the toes. One of these nerves may become irritated by the ligament located above it, causing it to become thickened and painful. Generally this problem occurs most often between the third and fourth toes, but it can occur between the second and third toes as well. It is uncommon for a neuroma to be located between the first and second or fourth and fifth metatarsals. Rarely is there more than one neuroma in a foot.
Causes
Unfortunately, the cause of Morton?s Neuroma remains unknown to researchers. It is likely that a variety of factors may play a role in the development of this condition, including the presence of chronic pain conditions like fibromyalgia. Factors that may contribute to the development of Morton?s Neuroma include Wearing improperly fitting shoes can cause pressure on your foot, leading to swelling around the toe nerves. High heels are of particular concern as they cause a large amount of weight to be shifted to the ball of the foot. Repetitive activities like jogging, walking, and aerobics can also place a lot of pressure on the feet. This could lead to Morton?s Neuroma. Having a previous foot or muscle injury may cause you to hold your foot in a poor position when walking, contributing to nerve inflammation. Some people are just born with poorly shaped feet. People with extremely low arches or "flat feet" may suffer from Morton?s Neuroma more than others.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
You should visit a doctor or podiatrist (foot doctor) if you have pain or tingling that does not stop. Your health care provider will examine your feet and will apply pressure on the spaces between the bones of the toes to determine the location of the foot pain. The doctor may order X-rays to rule out other conditions associated with foot pain, such as a stress fracture or arthritis. X-rays alone will not show whether or not a neuroma is present, so an ultrasound scan or magnetic resonance imaging (MRI) test may be done to confirm the diagnosis. A diagnostic procedure called an electromyography is sometimes used to rule out nerve conditions that may cause symptoms like those of associated with Morton?s neuroma.
Non Surgical Treatment
If you have Morton's neuroma, shoes with a wider toe area may be recommended. You can also take painkillers to help ease the pain. Steroid injections may also be given to treat the affected nerve. If these treatments don't work, surgery may be needed. This involves removing the thickened tissue around the nerve (and sometimes the nerve itself) to release the pressure.
Surgical Treatment
Recently, an increasing number of procedures are being performed at specialist centers under radiological or ultrasound guidance. Recent studies have shown excellent results for the treatment of Morton's neuroma with ultrasound guided steroid injections, ultrasound guided sclerosing alcohol injections, ultrasound guided radiofrequency ablation and ultrasound guided cryo-ablation.
The nerves located on the bottom of the foot between the metatarsal heads (the bone of the toe closest to the foot) supply feeling, or sensation, to the toes. One of these nerves may become irritated by the ligament located above it, causing it to become thickened and painful. Generally this problem occurs most often between the third and fourth toes, but it can occur between the second and third toes as well. It is uncommon for a neuroma to be located between the first and second or fourth and fifth metatarsals. Rarely is there more than one neuroma in a foot.Causes
Unfortunately, the cause of Morton?s Neuroma remains unknown to researchers. It is likely that a variety of factors may play a role in the development of this condition, including the presence of chronic pain conditions like fibromyalgia. Factors that may contribute to the development of Morton?s Neuroma include Wearing improperly fitting shoes can cause pressure on your foot, leading to swelling around the toe nerves. High heels are of particular concern as they cause a large amount of weight to be shifted to the ball of the foot. Repetitive activities like jogging, walking, and aerobics can also place a lot of pressure on the feet. This could lead to Morton?s Neuroma. Having a previous foot or muscle injury may cause you to hold your foot in a poor position when walking, contributing to nerve inflammation. Some people are just born with poorly shaped feet. People with extremely low arches or "flat feet" may suffer from Morton?s Neuroma more than others.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
You should visit a doctor or podiatrist (foot doctor) if you have pain or tingling that does not stop. Your health care provider will examine your feet and will apply pressure on the spaces between the bones of the toes to determine the location of the foot pain. The doctor may order X-rays to rule out other conditions associated with foot pain, such as a stress fracture or arthritis. X-rays alone will not show whether or not a neuroma is present, so an ultrasound scan or magnetic resonance imaging (MRI) test may be done to confirm the diagnosis. A diagnostic procedure called an electromyography is sometimes used to rule out nerve conditions that may cause symptoms like those of associated with Morton?s neuroma.
Non Surgical Treatment
If you have Morton's neuroma, shoes with a wider toe area may be recommended. You can also take painkillers to help ease the pain. Steroid injections may also be given to treat the affected nerve. If these treatments don't work, surgery may be needed. This involves removing the thickened tissue around the nerve (and sometimes the nerve itself) to release the pressure.
Surgical Treatment
Recently, an increasing number of procedures are being performed at specialist centers under radiological or ultrasound guidance. Recent studies have shown excellent results for the treatment of Morton's neuroma with ultrasound guided steroid injections, ultrasound guided sclerosing alcohol injections, ultrasound guided radiofrequency ablation and ultrasound guided cryo-ablation.
Shoe Lifts The Ideal Solution To Leg Length Discrepancy
There are two unique variations of leg length discrepancies, congenital and acquired. Congenital indicates you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental phases of aging, the brain picks up on the gait pattern and identifies some variance. Our bodies typically adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch isn't really abnormal, require Shoe Lifts to compensate and generally won't have a serious effect over a lifetime.

Leg length inequality goes mainly undiscovered on a daily basis, yet this problem is simply solved, and can reduce a number of incidents of lumbar pain.
Therapy for leg length inequality usually consists of Shoe Lifts . These are generally economical, generally costing below twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most common health problem impacting men and women today. Over 80 million men and women suffer from back pain at some point in their life. It's a problem that costs companies millions year after year as a result of time lost and output. Fresh and more effective treatment solutions are always sought after in the hope of reducing the economic influence this condition causes.

People from all corners of the earth suffer from foot ache as a result of leg length discrepancy. In most of these situations Shoe Lifts can be of very beneficial. The lifts are capable of relieving any discomfort and pain in the feet. Shoe Lifts are recommended by numerous skilled orthopaedic orthopedists.
To be able to support the body in a balanced fashion, feet have got a vital role to play. Inspite of that, it is sometimes the most overlooked zone in the body. Many people have flat-feet which means there is unequal force exerted on the feet. This will cause other parts of the body like knees, ankles and backs to be affected too. Shoe Lifts ensure that correct posture and balance are restored.
Leg length inequality goes mainly undiscovered on a daily basis, yet this problem is simply solved, and can reduce a number of incidents of lumbar pain.
Therapy for leg length inequality usually consists of Shoe Lifts . These are generally economical, generally costing below twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most common health problem impacting men and women today. Over 80 million men and women suffer from back pain at some point in their life. It's a problem that costs companies millions year after year as a result of time lost and output. Fresh and more effective treatment solutions are always sought after in the hope of reducing the economic influence this condition causes.
People from all corners of the earth suffer from foot ache as a result of leg length discrepancy. In most of these situations Shoe Lifts can be of very beneficial. The lifts are capable of relieving any discomfort and pain in the feet. Shoe Lifts are recommended by numerous skilled orthopaedic orthopedists.
To be able to support the body in a balanced fashion, feet have got a vital role to play. Inspite of that, it is sometimes the most overlooked zone in the body. Many people have flat-feet which means there is unequal force exerted on the feet. This will cause other parts of the body like knees, ankles and backs to be affected too. Shoe Lifts ensure that correct posture and balance are restored.
The Right Way To Prevent Calcaneal Spur

Overview
If you're feeling pain on the bottom of your foot near your heel, pain after exercise or activity, or pain first thing in the morning or after a long period of sitting, then you may have a heel spur. Heel spurs don't have a magic cure, but you can take steps to ease the pain and to eventually get rid of them.
Causes
Over-pronation (flat feet) is a common cause of heel spurs, but people with unusually high arches (pes cavus) can also develop heel spurs. Women have a significantly higher incidence of heel spurs due to the types of footwear often worn on a regular basis.

Symptoms
Heel spur and plantar fasciitis pain usually begins in the bottom of the heel, and frequently radiates into the arch. At times, however, the pain may be felt only in the arch. The pain is most intense when first standing, after any period of rest. Most people with this problem experience their greatest pain in the morning, with the first few steps after sleeping. After several minutes of walking, the pain usually becomes less intense and may disappear completely, only to return later with prolonged walking or standing. If a nerve is irritated due to the swollen plantar fascia, this pain may radiate into the ankle. In the early stages of Heel Spurs and Plantar Fasciitis, the pain will usually subside quickly with getting off of the foot and resting. As the disease progresses, it may take longer periods of time for the pain to subside.
Diagnosis
A Diagnosis of Heel Spur Syndrome is a very common reason for having heel pain. Heel pain may be due to other types of conditions such as tendonitis, Haglund's Deformity, Stress Fracture, Tarsal Tunnel Syndrome, or low back problems. A more common condition in children is Sever's Disease. The diagnosis is usually made with a combination of x-ray examination and symptoms.
Non Surgical Treatment
Podiatric Care for heel spur syndrome may involve keeping the fascia stretched out by performing exercises. Your doctor may also suggest for you to be seen by a physical therapist. You probably will be advised on the best shoes to wear or some inserts for your shoes. Your podiatrist may suggest that a custom made orthotic be made to allow your foot to function in the most ideal way especially if you have excessive pronation. A heel lift may be used if you have a leg length discrepancy. Medical treatment may include anti-inflammatory oral medications or an injection of medication and local anesthetic to reduce the swelling and decrease pain. If a bursitis is present the medication may greatly improve the symptoms. Your podiatric physician may also recommend a surgical procedure to actually fix the structural problem of your foot.
Surgical Treatment
Though conservative treatments for heel spurs work most of the time, there are some cases where we need to take your treatment to the next level. Luckily, with today?s technologies, you can still often avoid surgery. Some of the advanced technologies to treat a Heel Spur are Platelet Rich Plasma Therapy. Platelet Rich Plasma Therapy (also known as PRP) is one of several regenerative medicine techniques that University Foot and Ankle Institute has helped bring to foot and ankle care. This amazing in-office procedure allows the growth factors in the blood to be used to actually begin the healing process again long after your body has given up on healing the area. Heel Pain Shockwave Therapy. Shockwave therapy is a non-invasive procedure done in the office that allows for new blood to get to the region of fascia damage and help with healing. Results have been excellent with more than 70 percent of patients getting relief with only one treatment. Topaz for Heal Spurs and pain. Another minimally invasive technology technique is called Coblation Surgery using a Topaz probe. This minimally invasive procedure involves controlled heating of multiple tiny needles that are inserted through the skin and into the plantar fascia. This process, like PRP and Shockwave therapy, irritates the fascia enough to turn a chronic problem back into an acute problem, greatly increasing the chances of healing. Heel Spur Surgery. Endoscopic Plantar Fasciotomy is one surgical procedure that we consider to release the tight fascia. University Foot and Ankle Institute has perfected an endoscopic (camera guided) approach for fascia release to allow rapid healing and limited downtime with minimal pain.